For hiring teams, that convergence creates real pressure. Reactive, posting-based recruitment no longer works when candidates have multiple offers and employers across sectors are competing for the same finite pool.
This article breaks down the four most consequential NP recruitment trends heading into 2026—covering specialty-level demand concentration, the geographic impact of full practice authority expansion, how AI and telehealth are reshaping roles and sourcing, and what employers need to do differently to compete.
TL;DR
- NP employment is projected to grow 40% from 2024–2034, adding 128,400 jobs—double the PA growth rate and 13x the physician rate
- Psychiatric/mental health NPs are the hardest specialty to fill, commanding a $22,672 total compensation premium over Family NPs
- 27 states plus D.C. now grant full practice authority, reshaping where NPs choose to work
- 85% of psychiatric-mental health APRNs use telehealth, making virtual-first NP roles a mainstream expectation
- Flexible staffing models (contract, interim, and per diem) are now standard recruitment tools that employers rely on year-round
Key Trend 1: Record NP Demand and Specialization Concentration
The Growth Gap Is Real
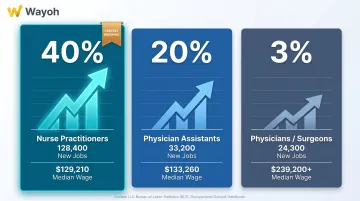
The scale of NP hiring pressure becomes clear when you compare provider categories side by side:
| Role | Growth Rate (2024–2034) | Projected New Jobs | Median Wage (May 2024) |
|---|---|---|---|
| Nurse Practitioners | 40% | 128,400 | $129,210 |
| Physician Assistants | 20% | 33,200 | $133,260 |
| Physicians/Surgeons | 3% | 24,300 | $239,200+ |
NP growth is double the PA rate and more than 13 times the physician rate. That gap isn't a short-term blip—it reflects two structural forces: a projected shortage of up to 86,000 physicians by 2036 (AAMC, 2024) and 75 million Americans living in primary care shortage areas with no adequate provider access.
Where Demand Concentrates
Not all NP specialties face equal pressure. Four categories consistently generate the longest vacancies:
- Psychiatric/Mental Health NPs (PMHNPs) — 122 million Americans live in a mental health HPSA; PMHNPs now fill 1 in 3 Medicare mental health prescriber visits
- Family NPs — The primary care access gap drives persistent demand, particularly in rural and underserved markets
- Geriatric NPs — The U.S. 65+ population grows from 58 million today to 82 million by 2050; all baby boomers will be 65+ by 2030
- Oncology NPs — Chronic disease burden (129 million Americans have at least one major chronic condition) keeps this pipeline tight
The mental health gap is especially acute. There are only 55,520 PMH-APRNs nationwide against a population of 122 million in shortage areas. For employers in behavioral health and healthtech, that supply-demand imbalance translates directly into longer vacancy windows and higher counter-offer rates.
Cross-Sector Competition Has Arrived
That scarcity is sharpened by a competitive landscape that now extends well beyond hospital systems. CVS Health/MinuteClinic, Amazon's One Medical, and a wave of healthtech startups are all recruiting Family NPs for technology-powered primary care, chronic disease management, and virtual-first care models. Many offer compensation and schedule flexibility that traditional systems simply can't match.
Employers relying on standard job postings are often the last to know a candidate was available — and the first to lose them.
Key Trend 2: Full Practice Authority Expansion and Hiring Geography
The 27-State Map That Shapes Recruitment
As of 2025, 27 states, Washington D.C., and 2 U.S. territories grant full practice authority (FPA) to NPs, allowing them to evaluate, diagnose, prescribe, and manage patient care independently without physician supervision. This is the model recommended by both the National Academy of Medicine and the NCSBN.
FPA matters for recruitment because autonomous practice is a genuine candidate preference—particularly for experienced NPs who have completed collaborative agreements and are ready to work independently.
The Three Largest NP Markets Are Still Restricted
Here's the tension: three of the highest-volume NP employment states have not adopted FPA.
| State | FPA Status | Key Detail |
|---|---|---|
| California | Reduced Practice | AB 890 created an independence pathway, but requires a transition period—not automatic FPA |
| Florida | Restricted | Physician supervision required; proposed SB 758 (2025) would only extend autonomy to certain psychiatric APRNs |
| New York | Reduced Practice | FPA legislation introduced but not enacted |
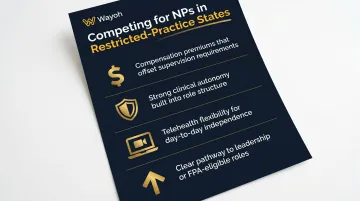
Employers in these markets face a real disadvantage when competing for candidates who specifically seek autonomous practice settings. That's not insurmountable, but it requires deliberate messaging. Effective offsets include:
- Compensation premiums that reflect the supervision requirement
- Strong clinical autonomy built into the role structure itself
- Telehealth flexibility to broaden day-to-day independence
- Clear career trajectory toward leadership or FPA-eligible positions
The APRN Compact: Watch This Space
The APRN Compact—which would allow NPs to practice across member states on a single license, similar to how the Nurse Licensure Compact works for RNs—has been enacted in only 4 states: Delaware, North Dakota, South Dakota, and Utah. It is not yet operational.
Six additional states have pending legislation, including Texas, Arizona, and Maryland. When the Compact activates, it will reduce credentialing delays for telehealth and distributed care teams — a direct benefit for any employer building multi-state NP capacity.
Key Trend 3: AI, Telehealth, and Flexible Staffing Reshaping NP Roles
Telehealth Is the New Standard—At Least for Psychiatric NPs
Among psychiatric-mental health APRNs, 85% now deliver care via telehealth, practicing across an average of two or more states. The majority work in outpatient and private practice environments rather than traditional hospital settings.
That's not a niche statistic. It means the fastest-growing, hardest-to-fill NP specialty has fundamentally restructured around virtual delivery. Employers who can't offer telehealth flexibility when recruiting PMHNPs are competing with one hand tied.
For other NP specialties, telehealth adoption varies, but the move toward virtual and hybrid models is consistent. Healthtech clients Wayoh works with—spanning digital care platforms, remote monitoring services, and preventative health programs—regularly recruit NPs specifically for roles where telehealth competency is a baseline expectation.
Technology Proficiency as a Job Requirement
NP workflows increasingly embed tools across several categories:
- AI-assisted clinical documentation and ambient scribing
- Multi-system EHR navigation and integration
- Remote monitoring platforms for chronic care management
- Predictive care tools tied to value-based outcomes
While no single authoritative survey quantifies exactly how many employers now specify tech proficiency in job postings, the pattern is consistent across virtual care, chronic care management, and digital health platforms.
NPs who can use these tools effectively—and work within compliant digital care workflows—are becoming a distinct hiring tier, bringing both clinical and operational value to technology-forward teams.
Flexible Staffing Is Now a Core Strategy
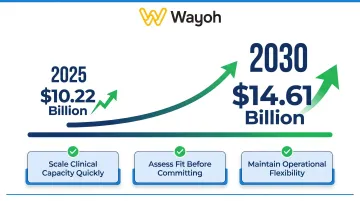
The locum tenens market is projected to reach $10.22 billion in 2025, growing to $14.61 billion by 2030. For NP hiring specifically, flexible arrangements—contract-to-hire, per diem, interim placements—have moved from gap-filler status to deliberate workforce strategy.
Healthtech startups and chronic care platforms are especially active users of flexible NP staffing. Full-time headcount commitments require board approval, budget cycles, and long onboarding timelines. Contract and interim arrangements let companies scale clinical capacity quickly, assess fit before committing, and maintain operational flexibility during growth phases.
Wayoh supports this model directly, offering interim, project-based, and contract placements alongside permanent and executive search. Candidates are vetted before introduction, and conversion terms are agreed upfront—no surprises when a contract role moves toward permanent hire.
How These Trends Are Reshaping NP Hiring Strategies
Move From Reactive to Proactive
The employers consistently winning NP talent aren't waiting for roles to open. They're building pipelines through:
- NP residency programs and new graduate pathways
- University and DNP program partnerships
- Professional association networks (AANP, APNA, specialty organizations)
- Ongoing passive candidate engagement before positions exist
That lead time matters because passive candidates—NPs who are employed and selectively open to the right opportunity—make up the majority of top-tier candidates in psychiatric and specialty roles. They don't apply to job postings.
Compensation Benchmarking by Specialty
Generic compensation packages lose specialty NPs. The data from the AANP 2024 Compensation Report is specific:
| NP Specialty | Mean Total Compensation |
|---|---|
| Psychiatric/Mental Health NP | $147,898 |
| Oncology/Hematology NP | $135,290 |
| Geriatric NP | $131,736 |
| Family NP | $125,226 |
| All NPs (mean) | $132,248 |
The BLS-confirmed median NP wage is $129,210 (May 2024), with the top 10% of APRNs earning more than $217,270. California leads state-level compensation at a mean of $166,018, compared to $115,586 in Alabama.
Compensation packages also need to account for bonus structure—42.2% of full-time NPs receive bonuses, most commonly tied to quality measures, RVU targets, or patient visit volume. Healthtech employers competing against hospital systems need to design packages that reflect both clinical and performance-based components.
Partner With Specialists Who Have Established NP Networks
Reactive posting and broad-reach job boards work for high-volume, low-specificity roles. For psychiatric NPs, specialty telehealth providers, and healthtech clinical hires, they fall short.
Recruiting firms with established NP networks bring advantages that job boards can't replicate:
- Surface qualified candidates who aren't actively applying
- Reduce time-to-fill for hard-to-find specialties like psychiatric NPs
- Provide compensation benchmarking that keeps offers competitive from the first conversation
Wayoh supports healthtech hiring through relationship-led search and vetted candidate pipelines built specifically for clinical and specialty roles.
Future Signals for NP Recruitment in 2026 and Beyond
Three developments will shape the NP hiring market over the next two to three years:
DNP enrollment growth may constrain future supply. DNP enrollment hit 44,976 students in 2024–2025, up 5.2% year-over-year across 452 schools. If DNP becomes an entry-level requirement — a direction AACN and NONPF have pushed for years without yet mandating it — the 12,207 annual DNP graduates become a bottleneck against 128,400 projected new positions. Employers should continue hiring MSN-prepared NPs now while monitoring policy momentum closely.
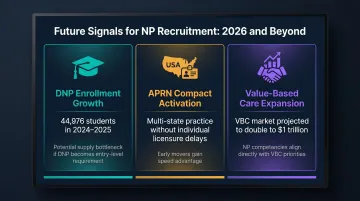
APRN Compact activation will change multi-state hiring speed. When the Compact reaches operational status, telehealth employers and distributed care teams can hire NPs across member states without individual licensure delays. Early movers who build compact-ready hiring infrastructure will gain a measurable cost and speed advantage over those caught flat-footed at activation.
Value-based care contracts will intensify NP demand. The VBC market is projected to grow from approximately $500 billion to $1 trillion. VBC models prioritize preventive care, chronic disease management, and care coordination — exactly the competency set NPs bring. As more health systems and employer health programs shift toward VBC contracts, NP hiring demand will grow in proportion.
Organizations that treat NP recruitment as a continuous investment — building talent pipelines, benchmarking compensation regularly, and working with recruiters who know healthtech's clinical and regulatory requirements — will have more resilient care teams than those responding to vacancies only when they appear. Wayoh works specifically within this space, placing NPs and clinical operations leaders for healthtech companies navigating these market shifts.
Frequently Asked Questions
How much does a nurse practitioner make in 2025?
The BLS-confirmed NP median annual wage is $129,210 as of May 2024. Specialty and location significantly affect earnings—psychiatric NPs average $147,898 in total compensation, and NPs in California or the Bay Area can exceed $200,000.
Which NP is most in demand?
Psychiatric/mental health NPs are the hardest to fill nationally, driven by 122 million Americans living in mental health shortage areas. Family NPs face sustained demand from the primary care access gap and physician shortage pressure.
Will NPs need a doctorate by 2025?
A DNP is not yet a universal licensure requirement—NPs can practice with an MSN in all states. Enrollment is rising (44,976 students in 2024–2025), and some employers prefer or require the DNP for leadership or specialized clinical roles, but it remains optional for practice.
Is hiring an NP worth it in 2025?
For healthcare and healthtech employers, NPs deliver quality care at significantly lower cost than physicians, with 40% projected job growth. That makes them a practical solution for organizations expanding primary care, mental health, or chronic disease management programs.
What states have the most NP job opportunities in 2026?
Per BLS data, the highest NP employment states are Texas, California, Florida, New York, and Tennessee. California and New York offer strong compensation but remain restricted-practice states, which can affect candidate preference and relocation decisions.
How can employers compete for top NP talent in a tight market?
The highest-impact moves are building your pipeline before a role opens, using specialty-benchmarked compensation rather than generic salary bands, and offering telehealth or flexible scheduling. Partnering with a firm like Wayoh—which maintains active NP candidate networks—gets you faster access to passive talent than job board postings alone.